This post is a big picture summary of all that’s happened since my cancer diagnosis. If you’re interested in all the details subscribe to email updates because I’m planning to post more regularly. The big decision points I’ll probably post to Facebook, otherwise I’m not going to announce every blog post on that platform. [Apologies, I cannot figure out how to add a subscription link into this post. Look for this icon: ]
I’ve done what feels like all the types of imaging that exist in the past month. And we went on a journey from “none of the doctors can feel a lump” which would indicate early stage cancer. To “actually this might be in your liver” which would indicate late stage cancer. Then landed back at “no spread other than one small local lymph node, and since there’s still no palpable lump even the cancer in your breast could be almost entirely in the ducts” – where cancer cells entirely contained within milk ducts would be stage 0 but spread to lymph nodes is more advanced than a localized tumor. So we’ve come full circle back to “we won’t know the stage or treatment plan until after surgery and pathology reports.”
On September 4 I will have surgery. It will be a double mastectomy with all the lymph nodes on the right side removed. I had my pre-op appointment Friday (August 15) and have been declared sufficiently healthy to be cleared for surgery. Now I get two entire weeks off from doctors appointments, which I don’t think has happened in years! (I’d been doing weekly appointments for at least one of: physical therapy, occupational therapy, vestibular therapy, and vision therapy since early 2023. Plus allergy shots every 3 weeks, massage every 4 weeks, and countless appointments with specialists or for testing.)
In the midst of all the cancer testing I moved out of my condo, sold it, rehomed my dog to one of the amazing employees at his daycare, and moved into an apartment that’s 5 minutes away from my parents house. Oh and I also had to coordinate transferring records and prescriptions and finalizing all the documentation for my disability insurance appeal while also doing all the regular paperwork associated with a move. I’m at a bit of a loss for what to do with my (very limited) energy since I haven’t had the choice to do anything but what’s absolutely necessary for what seems like forever. Two weeks to build routines in my new space and prepare for the next change in capacity is both a lot of time and no time at all. I’m planning for writing to be part of my new routine, so watch this space for more posts as I process everything that’s happened and write to organize my thoughts on what comes next.
I had my annual physical in December of 2024. At that appointment I pointed out that I would be turning 40 in a few months and requested to schedule a mammogram. My mom had breast cancer at age 61 so I didn’t qualify for early screening (they start screening 10 years before any family member was diagnosed, which for me was later than the standard start age) but I wanted to make sure I got in as soon as I qualified. I told the receptionist to make sure the appointment was after February so insurance would cover it, but they were booking into May regardless.
Had my mammogram in May. The tech told me it’s common to get called back for a follow up, especially after the first mammogram, so try not to worry if that happens. I did get called back. At that point I wasn’t worried. My body has always been weird. When I got an MRI to check for a cause of my headaches they found an abnormality in my Pituitary gland. After a few MRIs they’ve declared that abnormality not an issue and I don’t need to get it checked for 3 years. Turns out probably 25% of people have these spots but since most people don’t have a brain MRI they never know.
Follow up mammogram is in June. They have a great system where you get the mammogram, they send you to a waiting room (not back to the main waiting area thankfully), the doctor reads the images immediately to decide if they need any additional images, and then the doctor tells you the results. Gotta love a streamlined system. The doctor says the calcifications are localized which is a red flag and calcifications don’t show up on an ultrasound so the only way to check what’s going on is to go get a biopsy. Biopsy gets scheduled for June 25.
All the other life stuff happens. Puppy and I spend a week in Connecticut with my parents while the condo goes on the market. Offers are due June 24, we arrive home that afternoon. I go in for the biopsy Wednesday June 25. Accept one of the offers on the condo while sitting in the waiting room. They tell me to expect results the following week.
Friday afternoon I’m resting in bed, trying to recover from all the decisions I’ve been making, and I get a call. The biopsy results are ready, it is cancer, they’re very sorry but because of the July 4 holiday they can’t get me in for an appointment until July 9. On July 9 I’ll see a radiologist, an oncologist, and a surgeon. I hang up the phone and laugh.
I’m laughing because several people have said to me recently “that’s so much, you couldn’t have more going on simultaneously!”
I’m laughing because they apologized for a 12 day wait from results to appointments, plural! I’m used to waiting at least 6 months to see any specialist, 3 all at once is completely unheard of.
I’m laughing because I have a ton of big feelings and laughing releases them. I don’t have time to process anything because I need to leave right now to drive into Boston for Botox injections for migraine.
Since then I’ve cancelled all plans to move, seen all those doctors at the Danvers, MA Cancer Center, and also scheduled an appointment with a surgeon in CT near my parents. I have the most common and most treatable type of breast cancer (estrogen positive HER2 negative). It’s in a fairly large area (as many as 7 cm depending on who is reading the scans) but there’s no solid tumor.
Breast cancer treatment is nothing like any of my other chronic illnesses. They’re not going to guess what treatment might work (the only approach for trialing headache medications), they’re going to run a series of tests and work their way through a decision tree. I can make some decisions (double mastectomy vs single, research trial vs older protocol if I need chemo) but I don’t have to research my own diagnoses and advocate for treatment. It’s a completely different healthcare system than the one I’ve been existing in and it’s very refreshing.
Next step is an MRI on July 18 that will determine if we do chemo first (unlikely) or surgery first (more likely). I’ve scheduled the movers to put all of my belongings into storage on July 31 assuming that surgery is the next step and I’ll be recovering from that at my parents’ house. The movers were among the first 5 people I told about my cancer diagnosis – life has been really weird lately! After surgery I’ll find out what stage cancer and if I’ll need chemo or radiation. It’s possible I won’t need either and I’ll just take estrogen blocking medication, recover from surgery, and resume planning my cross country move. We’re hoping for that plan, I might actually make it out before winter in that case!
If you’re wondering what you can do after reading all that:
Take active steps to avoid catching and spreading disease. Learn about ventilation, stay home when you feel sick, and wear a mask in public spaces (you’re contagious before your symptoms start). People receiving cancer treatment are among the immunocompromised population. I wear an N95 respirator every time I go out, and masking is even more effective when everyone is doing it. There’s evidence that covid infections cause lasting damage, even in people who don’t experience long covid symptoms. This article discusses how covid may be inhibiting the body’s ability to eradicate cancer cells before they spread. https://www.washingtonpost.com/health/2024/06/06/covid-cancer-increase-link/
Support scientific research. Donate or call your Representatives or share your favorite research organization.
Send me simple distractions. It’s rather annoying to be sick and not able to watch TV, aren’t people who are stuck at home sick supposed to watch TV? My brain can’t handle that much input. Light audiobooks, funny podcasts, cute photos. I can do those.
This is a two part series, this post is part 1 and provides an update on what’s been going on with me lately. Feel free to skip straight to part 2, Cancer Diagnosis, if you’re up to date on the other stuff going on in my life.
Big picture recap:
July 2022: first covid infection, never got better.
Slowly added lots of new symptoms that are all associated with long covid.
First year of long covid I saw lots of doctors, did loads of tests, acquired many diagnoses, and started some treatments.
Second year of long covid most doctors had already reached the end of their knowledge and basically said I had to wait until the research caught up. So I participated in a bunch of research studies and tried out some other treatments.
Third year of long covid (which wraps up at the end of this month) has been much more about adapting to living with chronic illness, while still pursuing treatments with doctors who have any ideas left.
In February of 2025 I needed my “as needed” migraine meds 14 out of 28 days. The weather was constantly swinging from high to low pressure and then back again. My fatigue was worse in the cold because my body struggles with all forms of energy and staying warm uses a lot of energy. My pain was also worse with cold, tight muscles. I spent a week in Florida where I felt significantly better from a cold/pain/fatigue perspective, Florida did not help with the migraine situation. Once I realized that even 72 degrees and humid was still rather chilly for my body (I was sitting by the pool dressed in long sleeves and pants, using a towel as a blanket, while other people were lounging in bathing suits!) I was committed to the 2024-2025 winter being my last one in New England.
I reached out to friends and colleagues in Arizona and started planning my move. I spent a week in Arizona with my mom checking out neighborhoods around Phoenix. We went through all my belongings to minimize what would get shipped across the country. Posted on my local buy nothing Facebook group and distributed items to more than 40 families in my town (lots of messages coordinating pick up!). I scheduled condo repairs and updates and was about to put the place on the market when we got a ton of rain that then leaked through the windows. I scheduled more repairs and updates. Put the condo on the market and made plans to move myself, my dog, my car, and the rest of my stuff thousands of miles away.
Meanwhile:
February: long term disability declares me able to work full time (based on no actual evidence), start finding a lawyer to help file an appeal.
April: my daughter and her boyfriend moved out of the condo we were sharing. Dog starts having a lot more anxiety. Still working on disability appeal.
May: get laid off from my job (I’d been working ~10 hours per week). Dog still has anxiety, still working on disability appeal.
June: learn it’s very difficult to find a rental when I have no income and my dog is a pit bull mix. Dog still has anxiety, still working on disability appeal.
Despite disability insurance declaring me magically healed, I’m not, so I’m doing all this with about 4 hours available per day to do anything (the rest of the time I’m asleep or resting which means horizontal and nothing that requires too much concentration). I have to budget my physical, mental, and emotional exertion. Coordinating is mentally taxing and waiting for other people to help with the things I can’t do is stressful when I want to just get things done!
So that sets the stage. The last 6 months have been a lot. And… all that effort felt worth it because I was really looking forward to moving to my own place with a fenced in yard where it’s sunny all the time and once we survived the scorching months, it would be warm all the time too!
The NIH’s set of studies around long covid are called RECOVER (I assume it’s an acronym because it’s always in all caps? Edited 12/17 to add: found it in a The People’s CDC newsletter! “The Researching COVID to Enhance Recovery (RECOVER) initiative”). I’ve heard many concerns around the studies they’re doing, but they’re also the biggest funding source so I signed up hoping that at least some of the studies would be beneficial. The first step is to do a phone interview and some questionnaires to identify what symptoms I have. The official list for long covid has over 200 symptoms and everyone has a different subset. Once they have established a profile you can start enrolling in the specific studies.
A researcher in Boston is doing a study on sleep (aptly named RECOVER-SLEEP) with two different cohorts. One is for insomnia and the other is for hypersomnia.
The questionnaire to sort me into the sub-study asked about how much sleep I get, if it’s refreshing, and if I’m tired during the day. One of my concerns is there’s no differentiation between fatigue and feeling tired in the surveys. I’m always fatigued. I never feel refreshed upon waking. And I’m also not able to fall asleep during the day. I will occasionally struggle to fall asleep at night – especially after a day where I exerted beyond my capacity – but this isn’t a major symptom for me. I generally fall asleep easily, stay asleep a long time (at least 9 hours), wake up feeling fatigued, and force myself to rest throughout the day. I say force myself to rest because most days I’m capable in the moment of doing lots more than I can do without consequences. I get post exertional malaise (PEM) if I use more physical, mental, and emotional energy than my body can produce. This is the defining characteristic of myalgic encephalomyelitis (ME). So if I don’t force rest throughout the day I have more symptoms and increased severity of my baseline symptoms for the next few days. I honestly would rather be more tired if I have to have ME because it would make pacing easier.
Based on the questionnaire I was placed in the Hypersomnia sub-study. This makes sense since I’m sleeping more than the average person and still feeling fatigued.
I decided to enroll in this study since fatigue is one of my top 3 most debilitating symptoms and I was hoping the trial was for a treatment for long covid that would alleviate some of my fatigue. More specifically, I had assumed that the medication they were studying was trying to treat an underlying cause or condition that people with long covid have. After telling me I qualify for the hypersomnia study the research assistant described the medication as a stimulant. This set off red flags because I’m very sensitive to stimulants, and because if people who don’t understand ME feel more awake without resolving the actual disease that’s going to lead to a crash (small amounts of over-exertion result in PEM, continuing to push through PEM results in serious consequences like a decrease in baseline function and long term symptom flares).
I expressed my concerns right away to the research assistant. They didn’t know any more than the script in front of them so they arranged for me to speak to the lead researcher who is a doctor (the lead at the Mass General site, not at the NIH). While I was waiting for that conversation I was also able to review the consent form. It says “The study drug will be either modafinil (Provigil) or a placebo pill. Modafinil (pronounced mow-DAH-fuh-nil) is a pill taken by mouth and is used to help people to stay awake during the day.” As a reminder, I don’t need help staying awake. I’m awake all day, I have low energy while awake. The researcher said the drug exits your system quickly so if I have issues because I’m sensitive to stimulants I could stop taking it immediately and it would be cleared from my system in 12 hours. He also said that no one understands long covid chronic fatigue or post exertional fatigue and so the goal of this study is to see if this drug affects them.
In the moment that all sounded reasonable and so I signed the consent and we did the blood draw. I have a Garmin that helps me with pacing and I thought “I can withdraw immediately if things go the way I think they will.” But then during the car ride home I felt less sure.
I don’t like that he called it post exertional fatigue – I get lots more symptoms than fatigue if I overdo it. PEM is often described as “flu like symptoms” – it’s a whole set of symptoms including fatigue, muscle aches, congestion, sore throat etc. And my list of symptoms increases every few months. This spring I added an acidic feeling in my stomach to my PEM list, this fall I added pruned fingers (bodies are weird). I had flushing in my ears and face a few hours after I got home from the research visit from the exertion of driving and answering lots of questions (cognitive exertion requires a lot of energy).
While it’s true that long covid is new and we don’t have a lot of clarity on long covid chronic fatigue, it’s simply false to say we have no understanding to build from. Post viral illnesses are not new. ME is not new. Both have been significantly underfunded (see also: conditions that impact a much higher proportion of women than men) but they have been researched.
I’m not confident I won’t have a longer recovery time from any adverse reaction to the study drug. Most people may metabolize the drug quickly but my system is very fragile. I tried topomax for headaches over the summer and the raspy voice I developed as a side effect lasted months past when I stopped taking it.
If I’m on the placebo then I have to do 15 weeks of work for something I don’t think we should be spending energy studying.
All of that to say: I dropped out of the study after having more time to think. This decision was further validated when I asked my long covid discussion group about this study and someone found a research study on the drug they’re testing. I didn’t read the full study but right there in the abstract it says “The use of wakefulness-promoting agents is discouraged for addressing unexplained fatigue, as seen in the context of chronic fatigue syndrome.” (ME was originally called chronic fatigue syndrome before more research was done to understand that the mechanisms are related to muscle, brain, and inflammation – myalgic encephalomyelitis is those words in Latin/medical. The name chronic fatigue syndrome is still common among people who do not understand the extent of the condition.)
How did no one read that study before designing this clinical trial? At the very least there should be clearly stated risk factors. The risk factors in this consent form talk about how you might feel frustration while completing cognitive tasks and you might get a bruise from a blood draw. There’s nothing about the significant risk of increased symptoms if people believe themselves to be better and push beyond their actual capacity. I’m very concerned people who don’t realize they have PEM will be harmed by this study. I’m also concerned that the only people who stay in the study for a full 15 weeks will be people who have a type of long covid that doesn’t include PEM. If that happens, and there was no screening for PEM as part of enrollment, this study could be published as evidence this drug cures long covid fatigue. That is the most dangerous outcome as then doctors around the world could push this medication plus exercise on people who won’t know until they’re severely disabled that pushing through until burnout can be disastrous for people with ME.
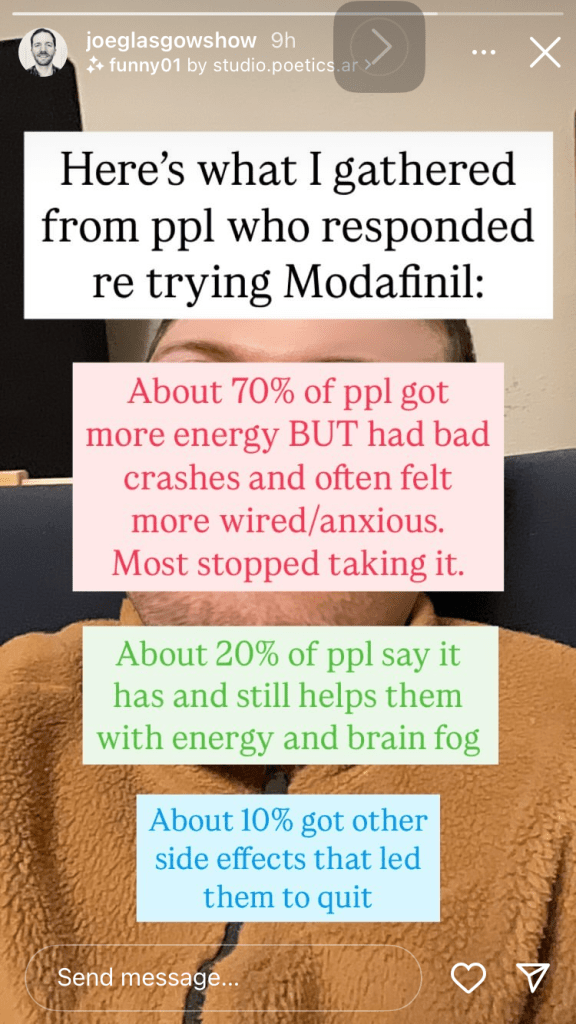
This concern is entirely based in reality. It’s already happening, as you can see from an informal survey done by someone with long covid on Instagram. A study backed by the NIH is only going to make this misinformation about how to deal with fatigue caused by long covid/ME more widespread.
Additional thought after I hit post the first time: The other cohort that has insomnia rather than hypersomnia seems less dangerous. They’re getting melatonin and light box therapy. They are still in the same boat of addressing a symptom without consideration of the underlying cause.
Email to the IRB:
All of the above plus: A member of my long covid discussion group reached out to their contact at the NIH after I posted, the contact said “The study co-chairs have been discussing this scenario and what education the sites need including clarity and language around the specific sleep phenotypes that RECOVER SLEEP is studying. The Project Leader is going to keep me updated on key discussion points and how the re-education of sites and support for participants is being carried out. I (and the study co-chairs) are thankful that this person reached out to you, and that you shared the email with me.” It is very concerning to me that the project leads have identified issues with the study and are continuing to recruit for it with complete disregard to the consequences.
Email to the local research team:
All of the above plus:
In addition to my concerns about the study at large, there are also things you can be doing to better support participants at your particular site. Everyone you are inviting to join the study has issues with sleep which automatically results in a level of cognitive impairment, and many folks with long covid have additional brain fog on top of that. Reducing cognitive load is essential for limiting the exertion required to participate.
Explain the parking and public transit options before people arrive (I did not know that the address you gave me landed me at valet parking.)
Explain the financial aspects (Do you validate parking? Reimburse for parking?)
Explain exactly how to reach the office (Do I check in at the front desk? Which elevator do I use?)
Estimate how long each appointment will be (I need to rest in advance and plan recovery time)
Ask about access needs (Participants may use a wheelchair to reduce exertion. I need text either read aloud or sent to my phone)
Doing any one of these things can help reduce the strain of participation. My symptoms increased after the appointment and it’s taken over a week for me to be able to write all of this, partially because of the PEM I faced after the appointment.
Suddenly last week my disability payment was over $1,000 less than it had been the previous month. I knew I’d started working more hours recently but I didn’t think that I’d worked enough to cause a big drop. I’d also increased my tax withholdings since I’d owed taxes this year, again, not enough to cause a big drop. So I emailed my disability insurance and asked what caused the difference.
Turns out, to celebrate my one year anniversary of being on long term disability, they changed the formula for how they calculate my disability payments.
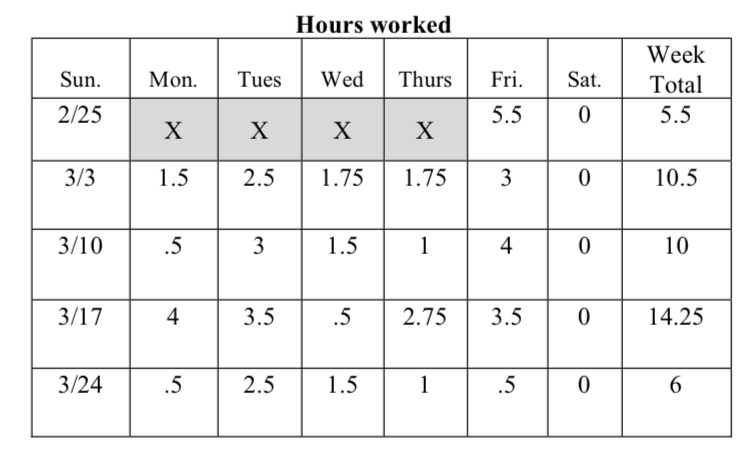
It used to be that disability paid 60% of my salary as of the date I went out on disability. I could earn additional money from my job by working part time and that didn’t impact my disability payment unless I earned more than 40% – makes sense I shouldn’t get paid more than 100%! They would have subtracted dollar for dollar any money I earned over 40% for the first year. This never happened. I’ve been working a couple hours a day on the days that I felt well enough and there was accessible work for me to do (primarily attending calls and answering questions on slack).
Now they’re deducting from my disability payment no matter how much I work. So I can earn more, but not as much more as last year. With this new system the total I earn per month between work and disability only increases $800 if I go from working 40 hours a month to 80 hours a month. My hourly rate is $44. 40*44=1760. I do not like this new math.
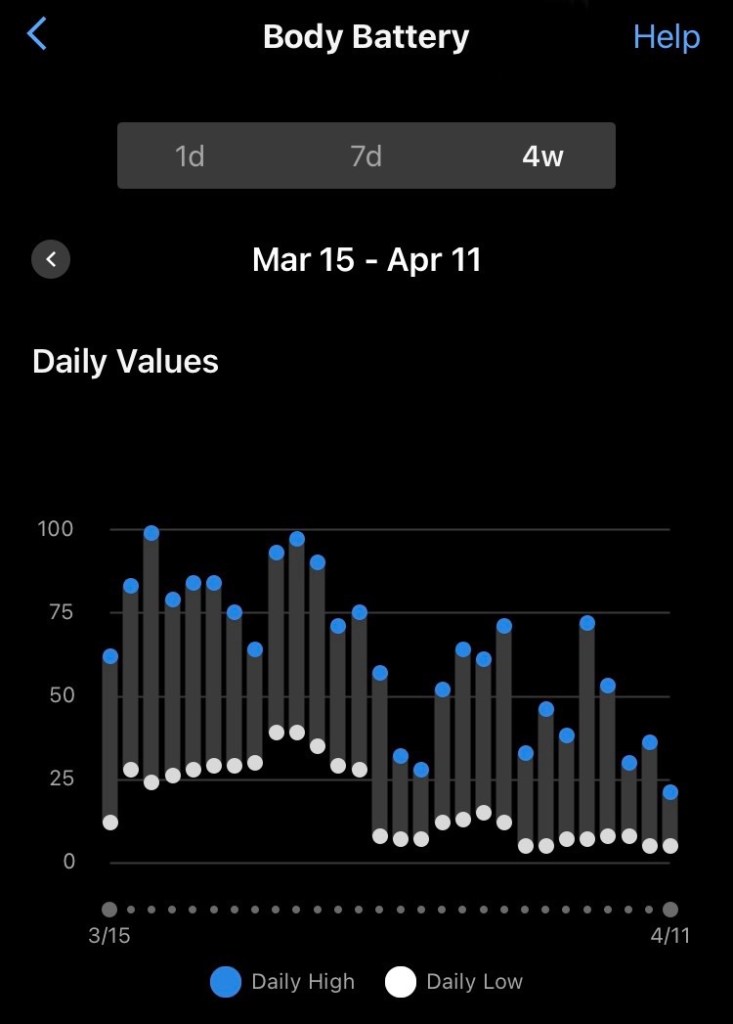
While this news has frustrating timing, it might help me not push too hard too fast. I’ve exited the initial stage of chronic illness where I spent all my time and energy going to doctors, collecting diagnoses, and trialing medications. The past month I’ve been relatively stable, able to stay home most days (traveling to appointments was physically and mentally draining), and begun focusing my attention on getting back to work. The past couple weeks I’ve been trying to figure out how to do editing tasks, when I’m still limited to my phone as the largest screen my eyes can handle. In the moment toggling and scrolling and memorizing and writing all feel fine. But based on my body battery scores, the nausea I feel when I take a break, and my lack of motivation to do anything but mindless scrolling on my evenings and weekends – my body isn’t ready for 4 hour work days.
My budget would really appreciate it if I could get back to earning the full salary I expected to have when I bought this condo, but there are other factors at play. And now that my disability insurance is decreasing the impact on my total income that working extra hours will have, I’m going to be even more careful about working within my energy envelope. Not the message disability insurance intended to send, I’m sure, but it’s the healthiest thing for me. And financially I’m privileged enough to be able to continue like this for a while. If I need to move to a more affordable area in the future, I’m ready to do that.
In the meantime I’m holding out hope that vision therapy will help. Last month they were accepting people added to the wait-list in November and I joined it in late January, so it’ll be a while until I can start, and many more months until we know if it will work. Until then, I’m going to try to be gentler with my straining eyeballs, inflamed brain, and poorly functioning mitochondria.
Long Covid Moonshot is asking everyone to contact their representatives, sharing your long covid story, and asking for funding for research into treatments and cures for the many facets of long covid.
I sent the message below to my representatives via democracy.io . Feel free to use any of what I said in your own message, including my story if you don’t have long covid yourself.
Tomorrow is long covid awareness day. March 28 will mark 19 months since my first, and only, covid infection. It will also mark 19 months of being out of work (I’m now on long term disability), of being too fatigued to leave the house most days, of being in unrelenting pain, and of wondering when everyone else is going to catch up with the science.
I have had an incredibly privileged experience with long covid – my family members are medical professionals, including a cardiologist and a neurologist (two of the main symptom groups people with long covid are facing), I live just outside of Boston which gives me access to an abundance of medical care, and I was working a job with benefits that included generous disability insurance. Even with all those privileges, I’ve seen too many doctors who have no idea how to help me, and I’m spending more money than I’m making between the cost of healthcare and the high cost of living here.
It’s past time for the government to take a stand against long covid. There is no cure, so the first priority is prevention. Reinstating funding for free PCR tests, at home rapid tests, and paid sick leave would make a huge difference in decreasing the spread of disease. Investing in clean air (via filtration, fresh air circulation, and other new tech) for the future, and high quality masking in the meantime is the only way we can move forward. Alongside prevention, there are millions of us who are already sick (1 in 15 Americans), we need both research and care. Many people are more sick than I am and need full time caregivers, the process to get paid care is far too convoluted and needs an overhaul. My insurance is denying to cover treatment options because they’re not proven – we need more research trials funded.
Long covid moonshot is calling for $1 billion per year, for the next ten years. If we don’t act now the entire world is going to be filled with disabled people, suffering from under researched conditions – post viral illnesses aren’t new, but they’ve never been given the attention they deserve, too often because these conditions impact women more often and more seriously, a group that has been seriously underrepresented in medical research.
I’ve been thinking a lot about joy, both in my personal and professional life. The vision of the organization I work for is to create a world where all students know, use, and enjoy mathematics. So recently we’ve been discussing how to better center the “enjoy” part of that phrase in our work. 15 months into significantly disabling chronic illness I’m also taking time to reflect on what joy looks like in the life I’m currently living. While my primary goal is to not get worse, that’s not my only goal. Just below that is a commitment to not wallow in grief over all the ways my life has changed. Chronic illness requires finding ways to live with symptoms. I can continue to trial new medications or treatments, and simultaneously spend my time adapting the rest of my life to fit within my current abilities.
If you asked me what brought me joy prior to getting long covid I might have said:
Puzzles, jigsaws and escape rooms and word games, board games
Reading
Going to movies or a show, watching TV
Work, writing
Learning new things
It’s felt like a lot of that is impossible, which it is. And, many of these moments of joy are still available on a smaller scale. I’ve reached the point where I’m okay with quieter moments of joy, I’m still enjoying my life even if it’s not the big flashy adventure it once was (this is half sarcastic, I’ve always been a deeply introverted homebody, and still true in comparison to how I’m living now). This shift feels like a normal part of aging, though my experience is certainly a case of my body limiting me younger and more significantly than is typical.
My puppy – we’re not going on hikes, exploring new places, or attending classes with other puppies. We’ve both settled down and enjoy quiet days on the couch with walks around the neighborhood and short play periods in the living room. He gets to go to daycare twice a week to run around. He’s still adorable and cuddly and surprises me with his intelligence. I appreciate his joyful bounce every time I offer him a treat.
I missed food on my first list, I also have a joyful bounce when I get myself a tasty treat! It doesn’t have to be at a restaurant (honestly they were mostly noisy which is strenuous for my hearing and my introverted self) – I can get takeout or make something or enjoy a meal someone else made for me. Opening my soup Wednesday delivery box each week is an exciting surprise since I’ve always forgotten what’s on the menu by the time it arrives.
Spending time with friends and their kids – this is often joy seeing photos of those kids rather than interacting with them directly. Spending time with friends is also a quieter event, sitting on my deck rather than going out. I really love my deck, today is one of the last warm days so I’m writing this outside.
Celebrating holidays with family – this requires advanced planning to space out travel, and we’ve skipped some of them, but now my parents come visit me a lot more often so we’re averaging more time spent together than previous years.
Hiking, especially letterboxing (https://www.atlasquest.com/) – there’s more time spent sitting outside than walking, and more time spent walking on flat ground than hiking. The trees are still pretty and the clouds are still fluffy. The goal is finding a photo to add to my instagram story rather than locating a stamp hidden in the woods. Still exciting to capture a good angle or to notice a new bloom.
Crafting, mostly crochet – this has been replaced by playing the guitar, crafting is too vision intensive and even a simple crochet pattern that I can do without looking requires some part of my brain (motor skills? imagining what it looks like?) that causes pain. I am also enjoying the graphic design that goes into Instagram posts and stories, some of which I create in Canva which is a fun creative outlet that I can engage in without having to repeatedly refocus my eyes.
Puzzles, jigsaws and escape rooms and word games, board games – I’m over 4,000 levels into a match 3 puzzle game. Not as exciting as completing a jigsaw puzzle, much more vision friendly. There are occasional escape room style puzzles to do on my phone (Timehop hosted a set of puzzles yesterday that I worked on with a friend) and word games (wordle, connections) are also sometimes acceptable to my brain.
Reading – I spend so much time listening to audiobooks.
Going to movies or a show, watching TV – again this has been replaced with audiobooks. It is really weird to have had so many “sick days” and spent none of them watching TV. This is the classic occupation of sick people. It’s visually painful and also audio description is too much for my brain (many people talking plus description plus soundtrack is overwhelming).
Work, writing – sometimes work is just frustrating to sit in meetings about things I can’t do, but work was never all joy. I’m ejoying the opportunity to discuss joy, to share my experiences, and to bring new perspectives in accessibility. Writing hurts my brain and I’m doing it anyway because it’s worth it! It’s nice to type on a keyboard again.
Learning new things – doing so much of that! All my science knowledge (okay, not all, I still haven’t used organic chemistry for anything, which doesn’t decrease the joy I experienced taking that class) has come in handy as I both attempt to understand what others have learned about my conditions and run my own experiments.
My new years resolution starting 2023 was to post a daily joy photo. I did for many days and then it started to feel fake. I was indeed finding joy in the sunny spot on my couch, or my neighbor’s flowers, or the particular way my puppy was sleeping. And I was also in pain, experiencing fatigue, frustrated with doctors not understanding my symptoms (that I’d learned all about and could diagnose!), and unable to do basic tasks without accommodations and rest. Now that we are approaching the end of 2023 (it’s November next week!) I’m embracing a both/and perspective. I can share the picture of the tree with bright red leaves, with text explaining how season changes impact my symptoms. I can turn a frustrating conversation where a doctor dismissed my concern into some speech bubbles on a pretty background. I’m still working on mindfully enjoying a cup of tea (I have a habit of putting the leaves in to steep, leaving the mug on the counter, and then forgetting to stand back up to do the next step) because as much of my day as I can spend not actively thinking about my symptoms, the better regulated my nervous system will be (which is as close to treatment as we get for dysautonomia until someone can identify what the underlying triggers are). And I can make my social media be an honest reflection of my reality. Luckily community building and education have always been my thing, so I truly do enjoy spending my time talking about all the new things I’ve learned about my body, disability, and the overlapping systems we live within.
Here’s to finding more joy going forward, and being honest about how that joy intertwines with the rest of our experiences. I listened to an audiobook, where a kid* said that it seems like adults feel more than one thing at a time. And as the book went on she was able to identify overlapping emotions she felt simultaneously. I love this as a characteristic of maturity – recognizing the complexity of living. (*It was Maya in the “Winter in Paradise” series by Elin Hilderbrand. If you end up reading it and find the quote please let me know!)
Recently, my employer announced that we would have Employee Resource Groups. They provided a list of example groups that employees could choose to join. At the announcement they offered “employees with disabilities” as one option. I was excited to sign up to lead that group! The following week when the google form went out asking us which groups we’d be interested in joining and leading, the title had changed to “differently abled.” My response was “I would like to lead the disabled group (which will not be called differently abled) and participate as an active member of the LGBTQIA+ group.” I’m curious who made the change, whether they are disabled, and why I had such a strong negative reaction to the switch.
I wrote a little bit about my identity as a disabled person in the Disability Pride Month post. As with any identity my understanding of it is constantly evolving, as I encounter new situations and learn more about both myself and the disability community. I’ve primarily been reading light, fun books – in 2020 when the world got scary I started reading exclusively romance novels. I needed the predictable structure to make books a fun distraction. I did make my romance novels a learning opportunity by always choosing books that centered characters from marginalized communities (including many disabled characters). As time passed I’ve added some more variety to the books I read, including some historical fiction and books for work, but I’m primarily using audiobooks as entertainment while I rest, which means they need to be cognitive rest too. I was excited to discover when the book Haben showed up in my Libby feed, that my brain could handle listening to it. It’s an engaging memoir of a deafblind disability rights lawyer and activist. Listening to this book helped me give language to the reaction I had to the phrase “differently abled.”
Quote from Haben (7:21 – I don’t do page numbers anymore, instead books are measured in hours and minutes) “Disability is not something an individual overcomes. I’m still disabled, I’m still deafblind. People with disabilities are successful when we develop alternative techniques and our communities choose inclusion.”
I wrote previously about how my parents couldn’t avoid discussing my allergies with me and how they made me different. However, we rarely discussed my other disability – my hearing impairment. It was identified at a kindergarten screening and my parents didn’t hide it from me, I knew why I had an annual audiologist appointment. They advocated for me to ensure I sat at the front of the classroom so that I could hear the teacher. And then that was it. Because my hearing is perfect in my left ear I never had any issues in our quiet house (that’s why it wasn’t identified until kindergarten). Neither of my parents had hearing issues (past tense because they both are of an age that they should be getting hearing screenings, go to the doctor if you’re reading this!) so when I didn’t complain of issues they generally forgot about my difficulty hearing and so did I.
When I was little I remember feeling So Frustrated playing a game of telephone with other kids. We sat in a circle and kids whispered a message from ear to ear. The person on my right whispered something in my right ear and I couldn’t understand a single syllable. I asked them to repeat the message and still understood nothing. Other kids encouraged me to just say whatever I heard, because the point of the game is for the message to get messed up bit by bit as it was passed along. Except I heard nothing. I eventually sat back and let the message be shared with the person on my left. Had we been playing the game counterclockwise rather than clockwise I wouldn’t have had an issue at all and would’ve had fun laughing along with everyone else. Had I remembered that I can’t hear any conversational tones out of my right ear, turned, and offered my left ear, I also would’ve been just fine. But I didn’t, because I forgot that the thing I go to an annual doctor appointment for might be relevant in any situation outside of that booth where I wear the tight headphones and they ask me to repeat words and raise my hand as I hear tones.
As I got older I started realizing there were spaces where other people could hear and I couldn’t. Much like the fact that I never realized my vision wasn’t perfect because I assumed no one could see faces across a cafeteria – everyone’s vision fades at some distance! – I also assumed that when I couldn’t hear it was hard for everyone to hear. (The fact that I sat in the front of the classroom for my hearing also aided in my late identification for needing glasses, I could see the board just fine from the front row!) In high school French class the teacher rearranged seats once in such a way that my left ear was directly next to the heater, which was noisily blasting hot air all class. I tried to explain to the teacher as he was assigning seats, but didn’t have the language to explain in French and he thought I wanted to sit next to my friend. After class I stated my case more clearly and firmly (in English) and the problem was resolved. By the time I got to college I couldn’t always remember which ear I could hear out of so I used the muscle memory of grabbing someone’s shoulder with my right hand and swapping them to my left side to remind me.
What does all of this have to do with the phrases disabled and differently abled? My hearing is an impairment. It is harder for me to hear than most people. I have very limited directional hearing (a skill that relies on two ears), I miss sounds that are only on my right side, and adding background noise makes my hearing even worse. The quantity or quality of my hearing doesn’t impact my value as a person. The fact that I can’t hear out of one ear does have an impact on how I interact with the world. I need the world to make accommodations for me. When I was teaching in a classroom I explicitly told the class on day one that they’d need to give me a visual signal when they wanted my attention because just calling my name left me oblivious to who needed help until I could recognize all of their voices (and even then it’s a lot easier to just follow the waving hand than to inspect each face to find the match to the voice). I was communicating that I had a disability and that I needed people to act differently.
Disability isn’t shameful, but it is real. I think that’s the heart of what upsets me about the phrase “differently abled,” it minimizes the reality that the world is built on assumptions about what humans can do, and every time someone falls outside that norm it takes effort to figure out how to provide access.
Let’s revisit that quote from Haben, “Disability is not something an individual overcomes. I’m still disabled, I’m still deafblind. People with disabilities are successful when we develop alternative techniques and our communities choose inclusion.”
I resonated with so many examples from the book. People asking “why didn’t you say something?” when you say that you didn’t hear them; because I can’t alert you to the fact that I had no idea you were speaking! Avoiding locations that are hard to hear (e.g. bars) and sitting back without trying to join the conversation when it becomes too exhausting to try. And then the novelty of someone who understands, who moves to a better location or speaks more clearly or asks what accommodations you’ll need. I’m excited to start the Employee Resource Group to have this conversation with colleagues with disabilities, and to share with the whole company ways that they can be better advocates for us. I’ll report back what we decide to name the group and what other resources we dive into together. In the meantime, go read Haben! It’ll take you less than 8 hours if you listen to it, or if you read at the same pace as the author speaks (it was extra cool to hear a memoir read by the author).
Pacing is the essential practice of conserving energy to prevent future symptoms. Lately I’ve been feeling more energetic (my new medication – Mestinon – is working!!) and so I have to re-evaluate my pacing plan. What new activities can I do? How long can I do them for? And how many activities in a day? The answer to each of these questions is dynamic, depending on the weather, the quality of sleep I got the past few days, the activities I’ve done recently, and some mysterious variables I have yet to identify.
When I first got long covid I woke up every morning feeling groggy. So when my physical therapist asked me each session if the exercises I’d done the previous session had caused Post Exertional Malaise (PEM – the hallmark symptom of ME/CFS) I said no. It wasn’t until I reached a point where I wasn’t treking to multiple appointments a week that I learned it was possible to wake up and feel just tired, not like I’d been dragged to the surface from a deep (and yet somehow not restful) sleep. I can now identify that I only get groggy when I don’t pace my activities well enough.
So I was surprised to find on Monday of this week that I woke up feeling terrible. In my groggy state I have to attempt to decipher what caused these increased symptoms, so I don’t accidentally repeat the activity. The chronic illnesses I have are cruel, they don’t communicate in the moment “hey, this is tiring.” Instead I get an alert “you overdid it!” anywhere from a few hours later to the next morning. Dysautonomia has a symptom called flushing, for me that shows up as what I have lovingly named “the red hot ear of overexertion.” It usually shows up in the evening while I’m resting on the couch, and it’s my first signal that I failed at pacing sometime during that day. Sometimes that’s the only consequence, blood is rushing to my head in a strange way, I apologize to my body, and then we continue on our way. Other times (like this week) that’s the first of several consequences. The rest of the symptoms wait until the next day to arrive.
I did have one additional clue on Sunday that I’d overdone it. When I went for a walk with a friend my Fitbit recorded the first 15 minutes of the walk as a walk, which is already a clue that this activity was more exertion than I have on a typical day. While I walk Brownie the dog twice a day, it involves so much stopping to sniff (and lately pausing to determine if Halloween decorations are safe to walk past) that my Fitbit doesn’t record it as a walk. But wait, there’s more! On Sunday my Fitbit counted the next 16 minutes of our walk as “Sport” – my heart rate got high enough that my watch was convinced I was doing some sort of exercise. This was perplexing since we continued walking, at a fairly slow pace, on flat ground, and then sat down on a bench at the end. On Sunday I assumed that my heart rate was high because I’d been upright for longer than I usually am (dog walks are 15-20 minutes) and that aggravated my POTS.
When I woke up not feeling well on Monday I attributed it to going for a long walk. I decided that I would rest the whole day, which was easy to do because Brownie goes to daycare on Mondays. So I would skip walking, physical therapy exercises, and guitar practice (sitting upright, reaching my arm, and focusing on my phone are all more exertion than lying on the couch). Then I promised myself I would go back to what I knew was safe – my physical therapy exercises that I do lying down, and seated rowing exercises – before attempting a long walk again.
On Tuesday I woke up feeling groggy again. This felt wrong. I’d gone on a walk by myself the previous week without the dog and that had included climbing a significant hill. My parents hypothesized that the missing variable was the pollen count. I do have fall allergies, and I took that walk without a mask, but I’ve had allergies my whole life and allergy haze feels different than PEM groggy. Wednesday was the same, and it was after I thought about the impact my therapy session had the previous week that everything finally clicked. Exertion in ME/CFS is physical, mental, and emotional exertion. The previous week I’d been drained after therapy, despite the fact that I’d sat still for the whole session, because emotional exertion counts. During the second half of that walk on Sunday? I was ranting about a frustrating situation. The combination of walking and talking and experiencing heightened emotions was what sent my body into a three day mini-crash. I finally figured it out!
It’s important to piece through the puzzle for a few reasons:
It’s really disheartening to be doing better and then inexplicably feel worse. I want to be able to do things and it sucks not knowing why I suddenly can’t.
If I know what caused the problem I can avoid doing it again.
Knowing what my body can’t do now allows me to plan for future activities. If I’m going to be having an emotional conversation I will make sure to do so seated and plan time to rest before and after. If I’m going for a walk I’ll set a timer to check my heart rate every 10 minutes and adjust as needed.
The puzzle of the Sunday walk is just one of the many puzzles I’m constantly trying to solve. Many of them are pacing – how far can I drive without consequences? Am I ready to restart cardio physical therapy? How much buffer time do I need to schedule in between work calls? I also have other puzzles, such as what cognitive activities can I handle? I’ve been successfully learning the guitar (for 15 weeks!) so I tried to add learning Spanish back into my routine. Immediate headache. Some days word puzzles are okay, other days not so much. Match 3 phone games go fine, timed levels on plants vs. zombies resulted in my body neglecting to breathe.
Having a chronic illness requires constant calculating of what my body can and cannot handle. Having multiple chronic illnesses makes the problem that much harder to decipher. Exercising is one of the most effective lifestyle changes to make for POTS, exercising is the most disabling thing for ME/CFS. Thankfully brain fog isn’t on my list of symptoms so I have a fighting chance of solving these puzzles and finding a safe path forward.